I believe with off-label, MDs could stay with the
Post# of 157745
(Total Views: 273)
Posted On: 03/27/2019 4:02:14 AM

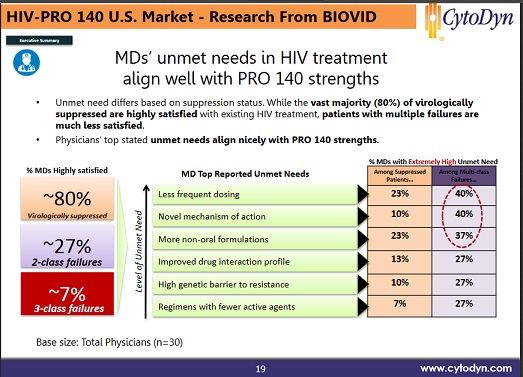
I believe with off-label, MDs could stay with the Combo regiment, but whenever a drug change is needed from bad side-effects, VL spike, or whatever, they might look at leronlimab with no SAEs, negligible toxicity, no documented resistance, and easy compliance; leronlimab matches what MDs have been looking in a new HIV drug. So not going as far as mono, but going beyond unmet need, and using with MDR1 patients. MDR1 is very big, 76%+ of HIV patients have at least one resistance. Also you see the MDR2 group has 27% highly satisfied, so a large percentage are interested in something new.
MDs survey n=30
Patient survey, n=20
MDs survey n=30
Patient survey, n=20
 (2)
(2) (0)
(0)