(Total Views: 642)
Posted On: 05/21/2025 9:08:48 AM
Post# of 157276

Re: StinkyPennies #153347
It’s all about market cap. CytoDyn’s float is a lot bigger, and I’m not trying to rain on anyone’s parade, just keeping expectations grounded.
At a current market cap of $5.8 billion, CytoDyn’s share price would be around $4.72, based on the 1.23 billion shares outstanding.
Compare that to RGC at $473 per share with a $6 billion market cap. That $473 seems like a floor for them, tied to the deal structure as far as I can tell. I think RGC might creep up a bit since $6 billion is the deal baseline, and their P/E looks low for a company with a licensing deal.
RGC’s deal was hefty, and it’s not totally out of reach for CytoDyn. Just a guess, but if we got a deal like that, I think we’d blow past $4 on the run up and maybe set a higher floor, thanks to our shareholder base and the known potential. We could see double digits for a short time, $10 or more wouldn’t shock me.
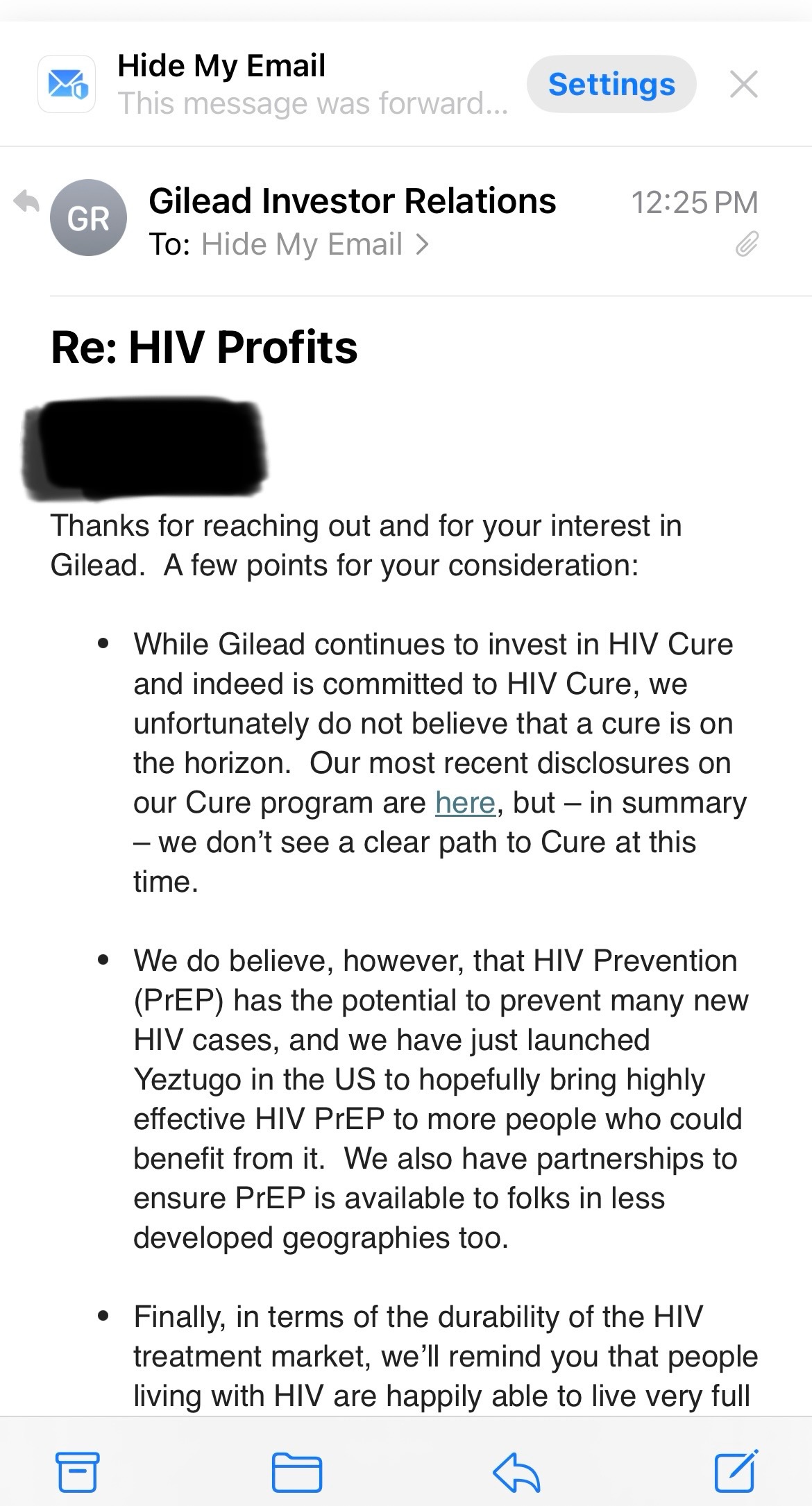
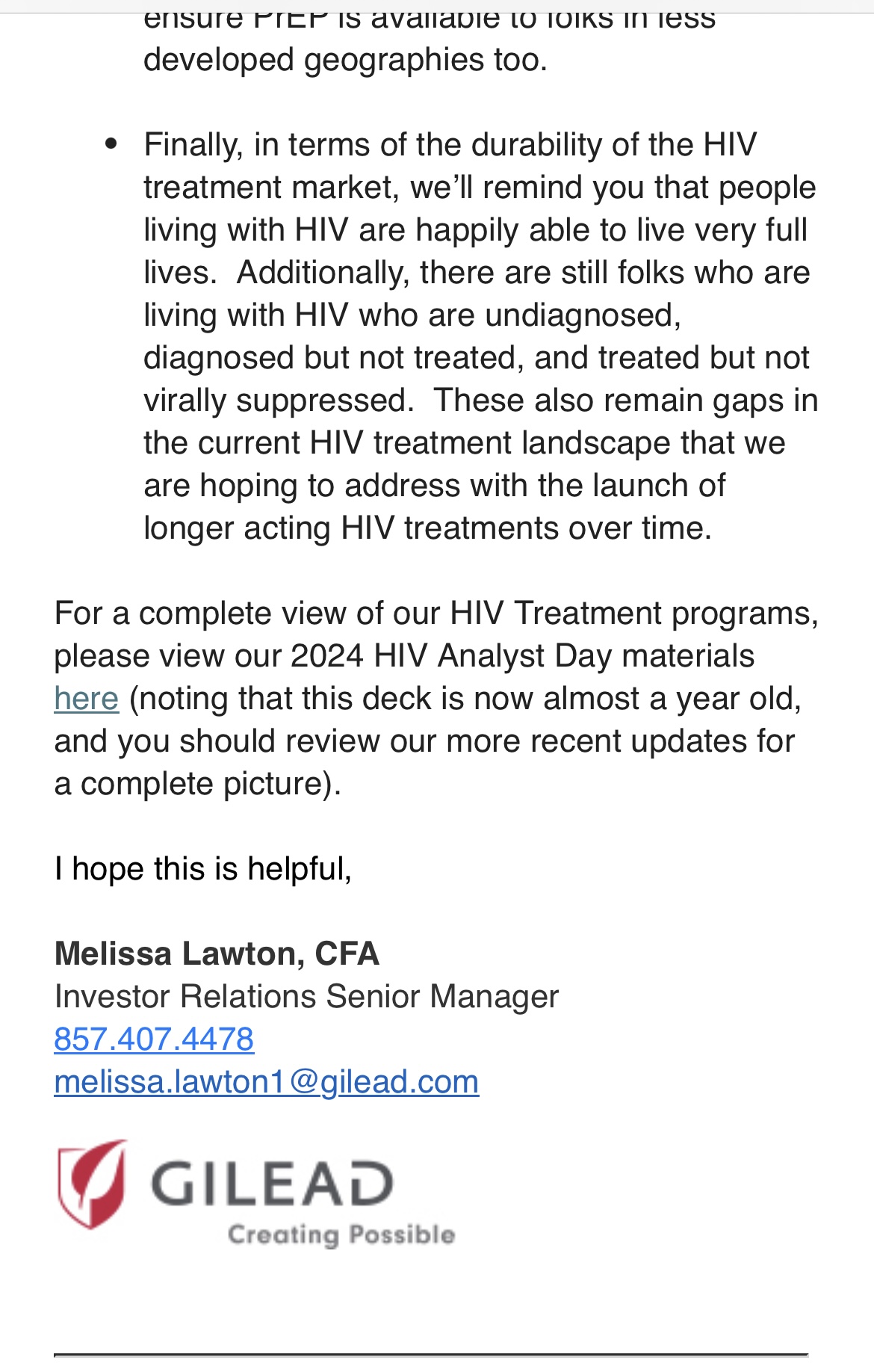
But there’s absolutely no way we hit $78 per share unless they drop some crazy PR, like curing 10 people of HIV with LATCH, and hype goes wild or POTUS/Gates says here’s the cure!
With a deal like this, the floor could become $4–$6, and most of should be very happy. That would hint at $10–$20 billion down the road, which is proving out what we always believed!
I’d probably sell a little on the way up, but we’d be way less risky with even just a $100 million plus licensing deal, which would probably cause a lot of de-risking too soon for many. Me personally I am a lot more risk adverse than I use to be.
It’s tough to say for sure, but sometimes companies explode, and the P/E could get inflated, even for us who’ve been here forever we might scream why did I sell at 8! Our P/E might push CytoDyn to $15 billion or more after a deal, wouldn’t shock me.
$70 Billon might make sense to some but it doesn’t at all to me unless there was some very unusual news within the next year or a meme stock event.
At a current market cap of $5.8 billion, CytoDyn’s share price would be around $4.72, based on the 1.23 billion shares outstanding.
Compare that to RGC at $473 per share with a $6 billion market cap. That $473 seems like a floor for them, tied to the deal structure as far as I can tell. I think RGC might creep up a bit since $6 billion is the deal baseline, and their P/E looks low for a company with a licensing deal.
RGC’s deal was hefty, and it’s not totally out of reach for CytoDyn. Just a guess, but if we got a deal like that, I think we’d blow past $4 on the run up and maybe set a higher floor, thanks to our shareholder base and the known potential. We could see double digits for a short time, $10 or more wouldn’t shock me.
But there’s absolutely no way we hit $78 per share unless they drop some crazy PR, like curing 10 people of HIV with LATCH, and hype goes wild or POTUS/Gates says here’s the cure!
With a deal like this, the floor could become $4–$6, and most of should be very happy. That would hint at $10–$20 billion down the road, which is proving out what we always believed!
I’d probably sell a little on the way up, but we’d be way less risky with even just a $100 million plus licensing deal, which would probably cause a lot of de-risking too soon for many. Me personally I am a lot more risk adverse than I use to be.
It’s tough to say for sure, but sometimes companies explode, and the P/E could get inflated, even for us who’ve been here forever we might scream why did I sell at 8! Our P/E might push CytoDyn to $15 billion or more after a deal, wouldn’t shock me.
$70 Billon might make sense to some but it doesn’t at all to me unless there was some very unusual news within the next year or a meme stock event.
Daniel Rizzo
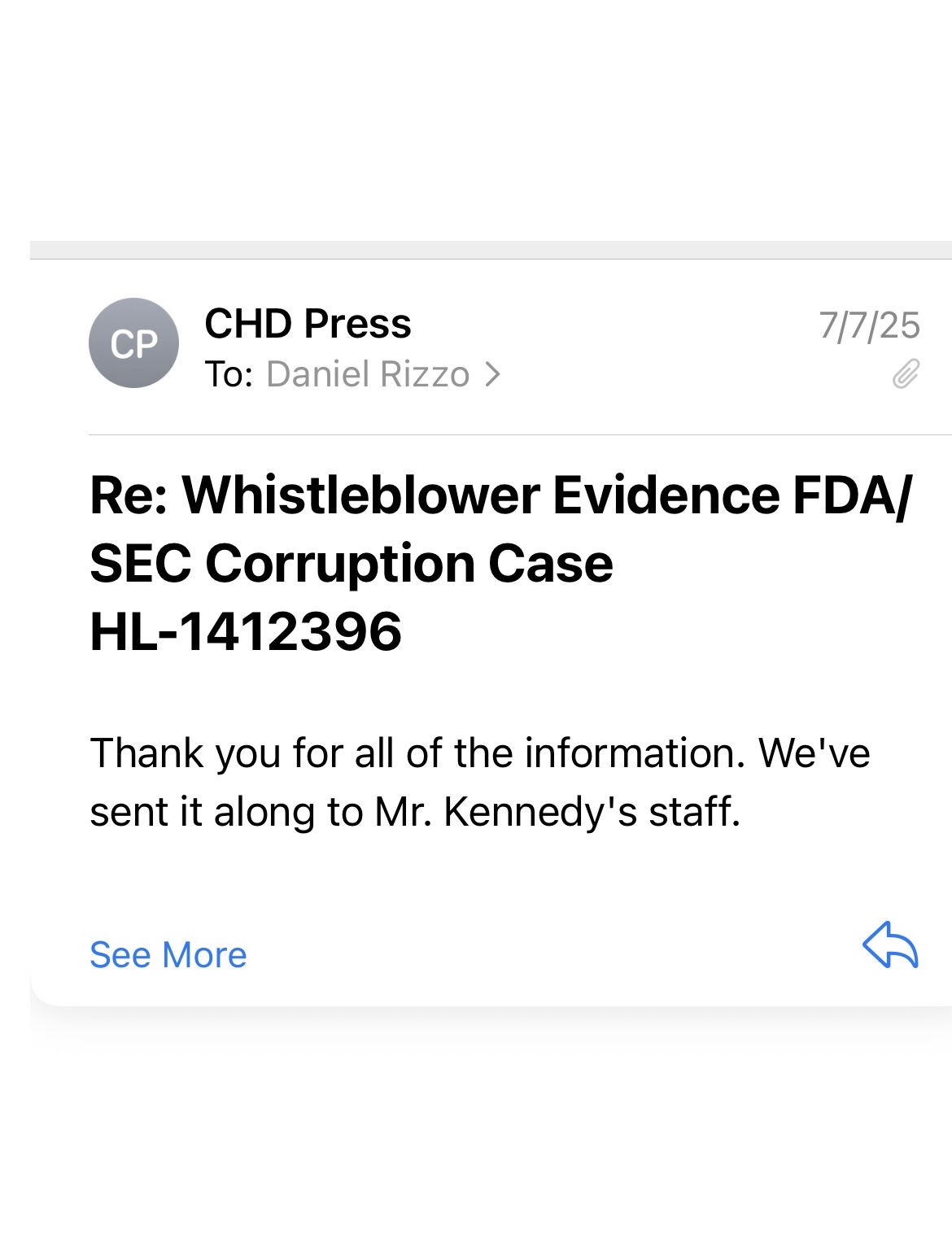
Federal Whistleblower
Case Numbers:
HHS & SEC Whistleblower: HL-1412396
DOJ Investigation Report/ Whistleblower ID: 20250705-0001
NIH Case Reference: CS1137565
DOD Case #16282
IC IG / 50 U.S.C. §3033
ARPA-H (Advanced Research Projects Agency for Health)
Founder & CEO of FireGate Bioscience
USPTO: Inventor of the HIV Cure Protocol
John 8:32 — “And ye shall know the truth, and the truth shall make you free.
NOTE….Digital forensics: Agencies already use SHA-256 hashes, mirrored storage, and chain-of-custody logs to prove evidence integrity. That’s standard practice in DOJ, FBI, SEC, etc.
• My system logs: They know ****** (and others) keep backend records that can be subpoenaed if needed.
• Blockchain provenance: Regulators (SEC, CFTC, even IRS) are familiar with timestamped ledgers and immutable audit trails.…
[/img]https://investorshangout.com/images/MYImages/1472647104_IMG_3103.png[/img]
https://investorshangout.com/images/MYImages/...G_2859.png
⸻
Public Links
FireGate Bioscience: https://www.firegatebioscience.com
NotYourDrug.com: https://www.notyourdrug.com
https://investorshangout.com/images/MYImages/..._3106.jpeg
https://investorshangout.com/images/MYImages/..._3107.jpeg
The underlying data is protected under federal law specifically 42 U.S.C. § 289b and its implementing regulation, 42 C.F.R. Part 93 through the Office of Research Integrity (askORI) within HHS, and coordinated with the Office of the Secretary / Office of Public Health and Science (OS/OPHS).
 - Waiting…
- Waiting…

whistleblower_complaints@wyden.senate.gov belongs to Senator Ron Wyden, a senior Democratic U.S. Senator from Oregon.
We are watching YOU……
“This isn’t conspiracy, this is criminal suppression.” - Ohm
https://www.justice.gov/usao-sdny/pr/us-attor...r-programs
https://investorshangout.com/images/MYImages/..._3015.jpeg
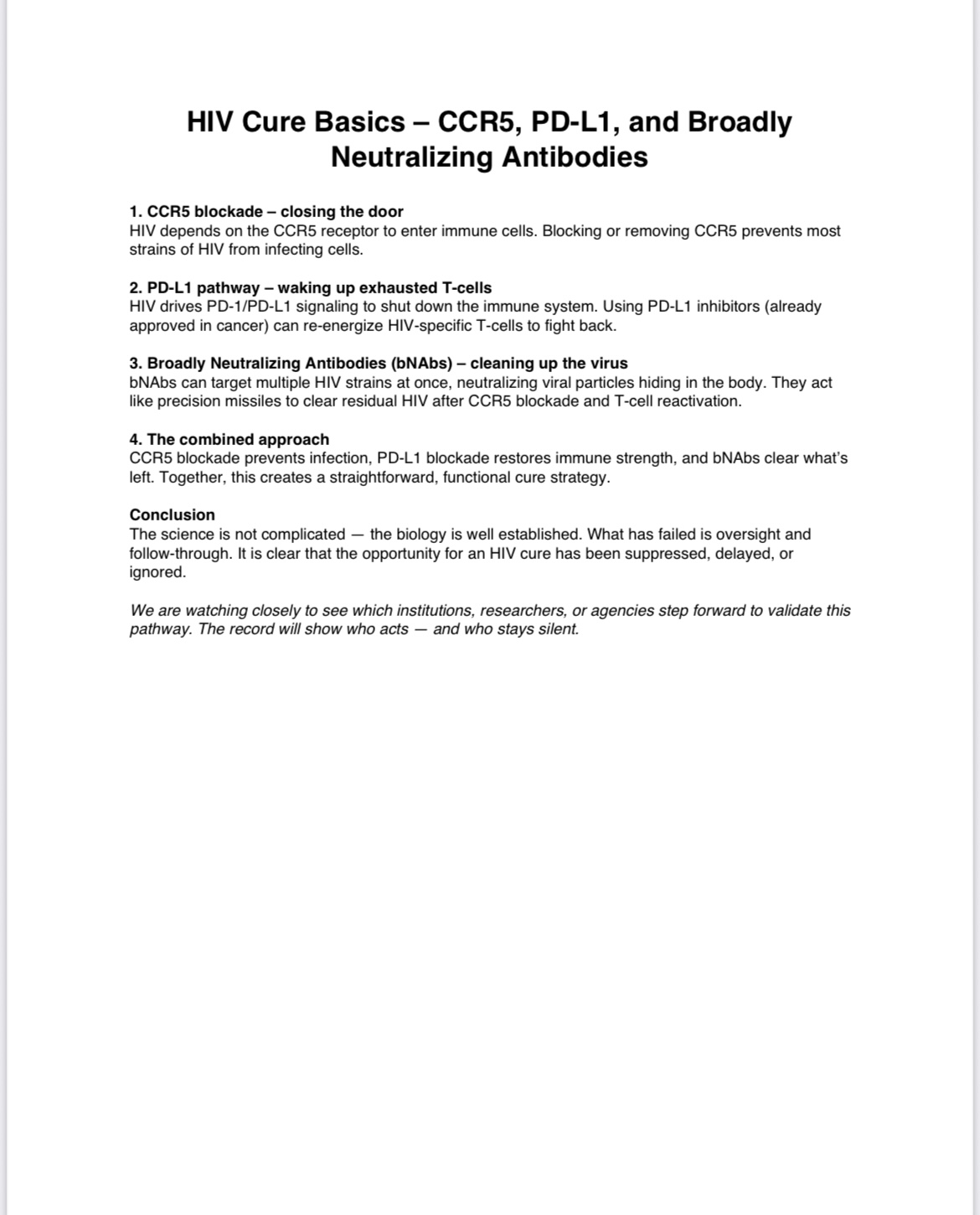
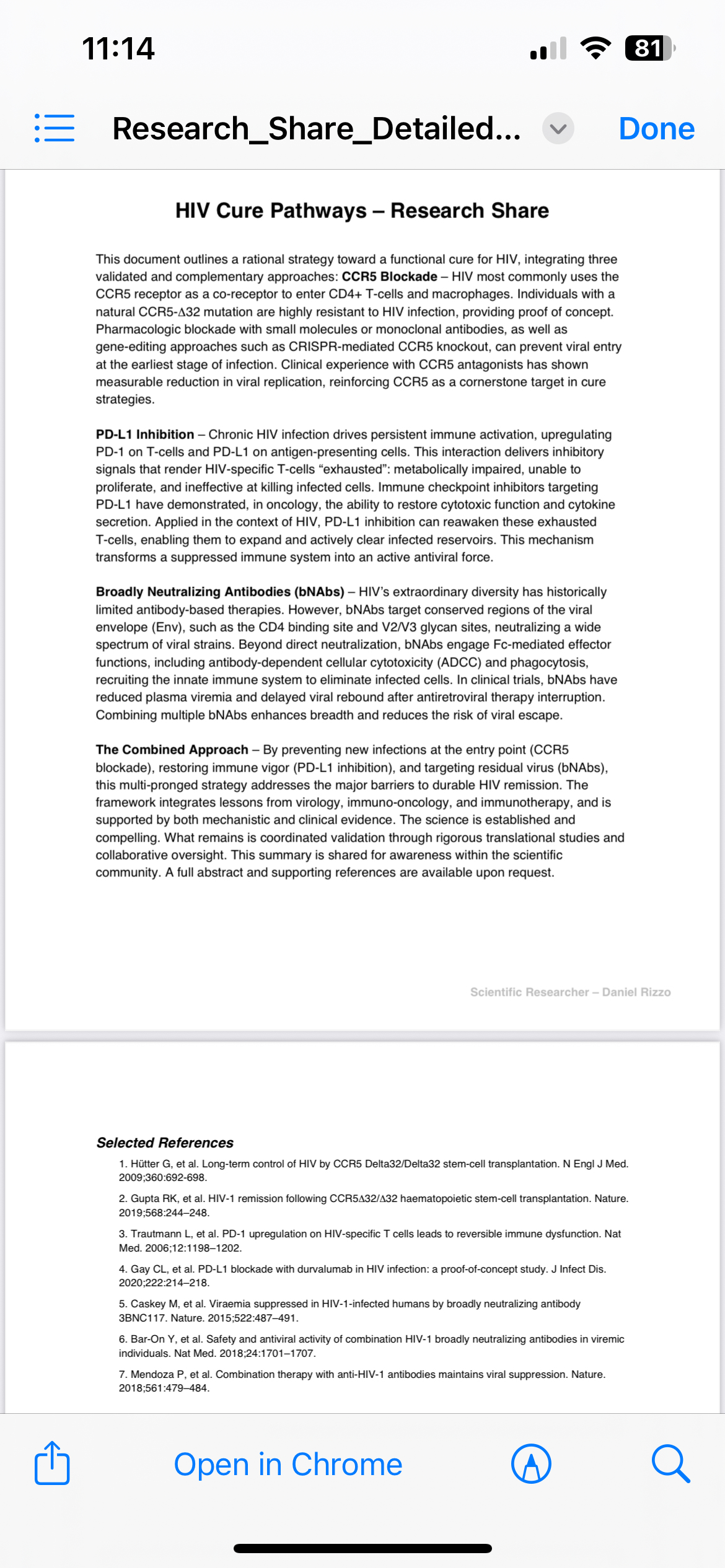
???? What Leronlimab Does
• Target: CCR5 receptor (the same receptor people with the CCR5Δ32 mutation lack — like the “Berlin” and “London” patients who were cured after stem cell transplants).
• Effect: By binding CCR5, leronlimab blocks HIV entry into CD4 cells.
• Trial Data:
• In combination therapy trials, ~81% of patients achieved viral loads <50 copies/mL (suppression, not cure).
• As monotherapy, some patients maintained suppression for long stretches (months), but not universally.
⸻
???? Why It Might Be Seen as a “Cure”
• In theory, if you completely block CCR5 on all relevant cells, HIV can’t infect new cells.
• If existing infected reservoirs naturally decay without replenishment, the virus could eventually vanish.
• That’s exactly what happened in the Berlin/London patients — except through stem cell transplants with CCR5Δ32 donors, not a drug.
⸻
???? Why It Hasn’t Been Called a Cure (Yet)
1. HIV Reservoirs Persist
Leronlimab blocks new infection, but it doesn’t flush latent virus from cells. Once treatment stops, those reservoirs can reignite infection.
2. CCR5-Independent Pathways
Some HIV strains use CXCR4 or dual-tropism (CCR5 + CXCR4). Leronlimab won’t stop those.
3. Clinical Conservatism
Researchers avoid using the word “cure” unless patients remain off all therapy with no viral rebound for years. Leronlimab hasn’t shown that in trials.
⸻
???? So Could It Alone Cure HIV?
• In select cases (if someone’s virus is purely CCR5-tropic and their reservoirs naturally decay): maybe.
• But in the general population, it’s unlikely as a monotherapy cure. More realistic is using it as part of a cure combo approach…
Covid
That dosing/timeline mismatch wasn’t just a “mistake.” It sabotaged the trial.
• Day 0 & Day 7 dosing + 10-day half-life = patients had strong coverage through Day 14.
• But the FDA chose Day 28 as the evaluation point……. after drug levels had waned.
• That’s not science. That’s setting the bar where the drug was least likely to shine.
Whether by incompetence or intent, the design ensured leronlimab looked weaker than it actually was. That’s sabotage …..and the community knows it.
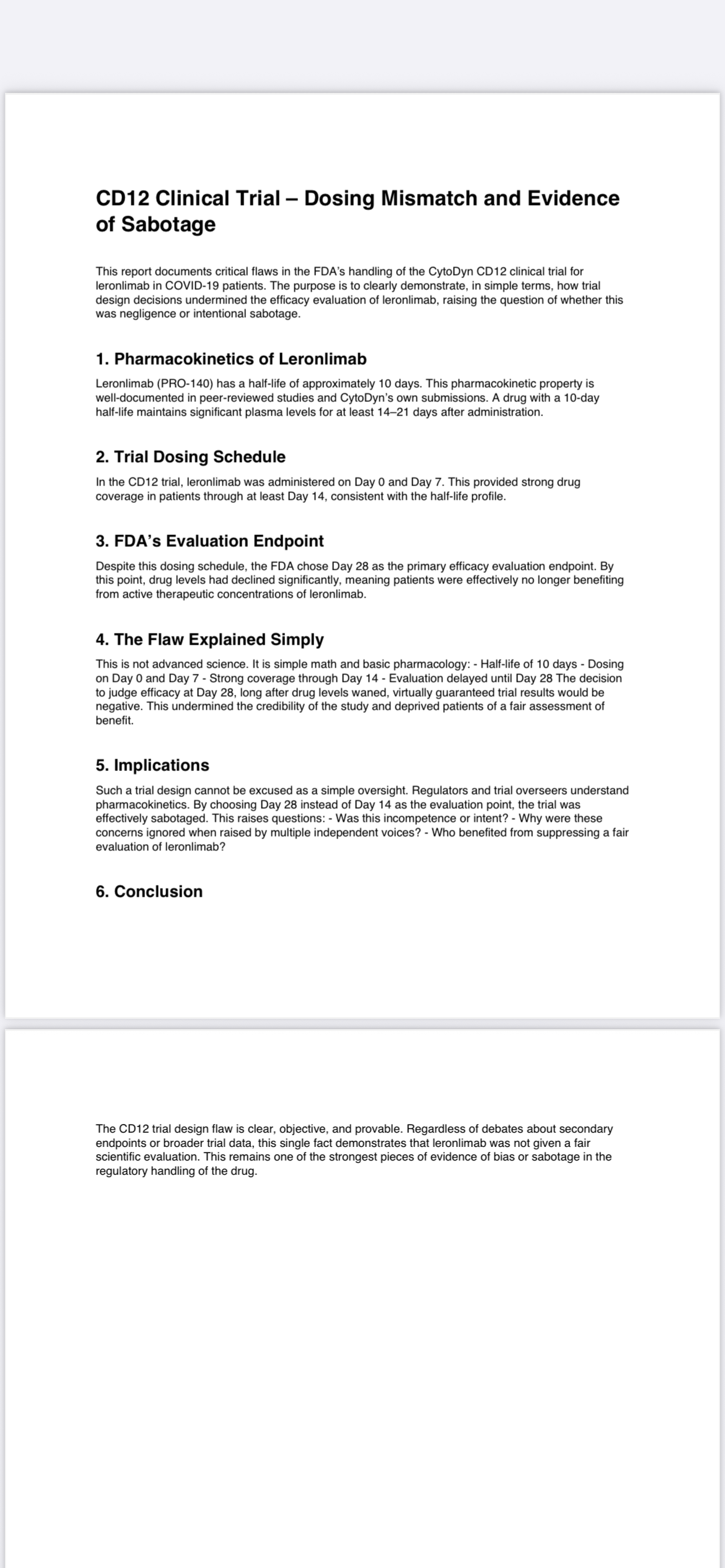
In 2020–2021, during CytoDyn’s CD12 trial of leronlimab (PRO-140) in severe/critical COVID-19 patients, the company requested FDA approval to amend the trial design. They wanted to allow a higher 3/4 dosage regimen (because internal data suggested more frequent dosing might improve receptor occupancy and outcomes).
• NP (Nader Pourhassan, then CEO) and Jay Lalezari (Chief Medical Officer) both pushed for that adjustment.
• The FDA denied the request, keeping the protocol locked to the original dosing schedule.
• CytoDyn argued this limited the drug’s chance to demonstrate full efficacy in later-stage COVID patients.
• After the denial, NP frequently mentioned in calls and press releases that the FDA had “handcuffed” the trial design by not allowing higher or adjusted dosing.
So yes….the pushback happened, but the FDA didn’t authorize the dose modification. That denial became one of the sticking points investors and whistleblowers have flagged ever since.
Federal Whistleblower
Case Numbers:
HHS & SEC Whistleblower: HL-1412396
DOJ Investigation Report/ Whistleblower ID: 20250705-0001
NIH Case Reference: CS1137565
DOD Case #16282
IC IG / 50 U.S.C. §3033
ARPA-H (Advanced Research Projects Agency for Health)
Founder & CEO of FireGate Bioscience
USPTO: Inventor of the HIV Cure Protocol
John 8:32 — “And ye shall know the truth, and the truth shall make you free.
NOTE….Digital forensics: Agencies already use SHA-256 hashes, mirrored storage, and chain-of-custody logs to prove evidence integrity. That’s standard practice in DOJ, FBI, SEC, etc.
• My system logs: They know ****** (and others) keep backend records that can be subpoenaed if needed.
• Blockchain provenance: Regulators (SEC, CFTC, even IRS) are familiar with timestamped ledgers and immutable audit trails.…
[/img]https://investorshangout.com/images/MYImages/1472647104_IMG_3103.png[/img]
https://investorshangout.com/images/MYImages/...G_2859.png
⸻
Public Links
FireGate Bioscience: https://www.firegatebioscience.com
NotYourDrug.com: https://www.notyourdrug.com
https://investorshangout.com/images/MYImages/..._3106.jpeg
https://investorshangout.com/images/MYImages/..._3107.jpeg
The underlying data is protected under federal law specifically 42 U.S.C. § 289b and its implementing regulation, 42 C.F.R. Part 93 through the Office of Research Integrity (askORI) within HHS, and coordinated with the Office of the Secretary / Office of Public Health and Science (OS/OPHS).
- Waiting… whistleblower_complaints@wyden.senate.gov belongs to Senator Ron Wyden, a senior Democratic U.S. Senator from Oregon.
We are watching YOU……
“This isn’t conspiracy, this is criminal suppression.” - Ohm
https://www.justice.gov/usao-sdny/pr/us-attor...r-programs
https://investorshangout.com/images/MYImages/..._3015.jpeg
???? What Leronlimab Does
• Target: CCR5 receptor (the same receptor people with the CCR5Δ32 mutation lack — like the “Berlin” and “London” patients who were cured after stem cell transplants).
• Effect: By binding CCR5, leronlimab blocks HIV entry into CD4 cells.
• Trial Data:
• In combination therapy trials, ~81% of patients achieved viral loads <50 copies/mL (suppression, not cure).
• As monotherapy, some patients maintained suppression for long stretches (months), but not universally.
⸻
???? Why It Might Be Seen as a “Cure”
• In theory, if you completely block CCR5 on all relevant cells, HIV can’t infect new cells.
• If existing infected reservoirs naturally decay without replenishment, the virus could eventually vanish.
• That’s exactly what happened in the Berlin/London patients — except through stem cell transplants with CCR5Δ32 donors, not a drug.
⸻
???? Why It Hasn’t Been Called a Cure (Yet)
1. HIV Reservoirs Persist
Leronlimab blocks new infection, but it doesn’t flush latent virus from cells. Once treatment stops, those reservoirs can reignite infection.
2. CCR5-Independent Pathways
Some HIV strains use CXCR4 or dual-tropism (CCR5 + CXCR4). Leronlimab won’t stop those.
3. Clinical Conservatism
Researchers avoid using the word “cure” unless patients remain off all therapy with no viral rebound for years. Leronlimab hasn’t shown that in trials.
⸻
???? So Could It Alone Cure HIV?
• In select cases (if someone’s virus is purely CCR5-tropic and their reservoirs naturally decay): maybe.
• But in the general population, it’s unlikely as a monotherapy cure. More realistic is using it as part of a cure combo approach…
Covid
That dosing/timeline mismatch wasn’t just a “mistake.” It sabotaged the trial.
• Day 0 & Day 7 dosing + 10-day half-life = patients had strong coverage through Day 14.
• But the FDA chose Day 28 as the evaluation point……. after drug levels had waned.
• That’s not science. That’s setting the bar where the drug was least likely to shine.
Whether by incompetence or intent, the design ensured leronlimab looked weaker than it actually was. That’s sabotage …..and the community knows it.
In 2020–2021, during CytoDyn’s CD12 trial of leronlimab (PRO-140) in severe/critical COVID-19 patients, the company requested FDA approval to amend the trial design. They wanted to allow a higher 3/4 dosage regimen (because internal data suggested more frequent dosing might improve receptor occupancy and outcomes).
• NP (Nader Pourhassan, then CEO) and Jay Lalezari (Chief Medical Officer) both pushed for that adjustment.
• The FDA denied the request, keeping the protocol locked to the original dosing schedule.
• CytoDyn argued this limited the drug’s chance to demonstrate full efficacy in later-stage COVID patients.
• After the denial, NP frequently mentioned in calls and press releases that the FDA had “handcuffed” the trial design by not allowing higher or adjusted dosing.
So yes….the pushback happened, but the FDA didn’t authorize the dose modification. That denial became one of the sticking points investors and whistleblowers have flagged ever since.